Uncategorized
Pharma’s Trial Problem: Outdated Systems, Broken Data, and the Coming AI Reset


Managing Director
Silicon Foundry, a Kearney Company
Clinical development has become the most resource-intensive stage of drug innovation. Across the industry, clinical trials consume 60–70% of total R&D spending, a proportion that continues to rise as trials grow more complex, more data-heavy, and more operationally demanding. The irony is that while science has advanced dramatically, the underlying model for running trials still reflects assumptions from a pre-digital era. The result is an ecosystem in which timelines stretch, costs multiply, and meaningful efficiency gains remain elusive.
AI has reached a level of maturity capable of reshaping this landscape, but its potential remains constrained by a fundamental issue the industry has been slow to confront. The data used to power these systems was never designed with AI in mind. In fact, the true crisis in clinical development today is structural and deeply rooted in how trial data is organized, contextualized, and interpreted.
Why trial models are failing
Clinical trials were built for physical sites, paper workflows, and slow-moving systems. Modern trials look nothing like that. They are distributed, data-heavy, biomarker-driven, and increasingly adaptive, yet they still run on infrastructure designed for a simpler era.
For years, clinical operations have been organized around sites and checklists rather than continuous insight. Data moves in bursts, workflows remain fragmented, and systems rarely talk to one another. Precision medicine expanded what trials could ask of data, but the way trials actually operate has barely evolved.
The problem isn’t only speed or scale. It’s also the quiet erosion of efficiency in places trial plans rarely account for. Across the industry, leaders describe a growing layer of “invisible waste”: repeated handoffs, duplicative manual work, incompatible data structures, and everyday operational friction that steadily stretches timelines and drives up costs, even though it seldom appears in formal project plans.
AI changes the equation, but only if trial data can support it.
Why AI stumbles in pharma
There is no shortage of AI talent, tools, or ambition in the life sciences sector. What is scarce is data that AI can meaningfully learn from. Most early AI-for-clinical-trials initiatives failed not because the models were immature, but because the data they were fed was not curated with clinical intent.
Two challenges define this crisis:
1. General-purpose models cannot interpret clinical nuance.
Models trained on large public corpora can identify patterns, but they lack clinical judgment. If the data is unstructured, inconsistently labeled, or lacks contextual metadata, the model will draw the wrong conclusions with absolute confidence. The well-known “ruler problem”—in which an AI system learned to detect malignant skin lesions based on the presence of a ruler beside the lesion—illustrates how easily models latch onto irrelevant signals.
2. Pharma’s internal data is both rich and unusable.
Organizations hold decades of trial data, but these assets are rarely AI-ready. Different study teams, CROs, and geographies used different standards. Biomarker and imaging data are often stored in systems that cannot communicate with EDC or safety platforms. And clinical notes, PDFs, and unstructured documents require interpretation that models cannot perform without curated training sets.
AI amplifies the quality of the data it is given. If the input is clinically inconsistent, overgeneralized, or disconnected from the trial context, the outputs will be clinically meaningless.
Recognizing this, many pharmas are now investing heavily in curated internal datasets, governance frameworks, and senior AI leadership, often in the form of newly created chief AI officer roles. These leaders are tasked with not just deploying tools, but rebuilding the data infrastructure from which future AI insights will emerge.
The new AI toolkit for clinical trials
Once the data foundation is strong, AI becomes a force multiplier across the entire trial lifecycle. Several categories show particularly high near-term impact potential.
Clinical-grade language models: Purpose-built models that ingest curated internal datasets can help draft protocols, refine eligibility criteria, flag operational risks, and interpret historical trial performance. Unlike general-purpose systems, these models are tuned to reason the way experienced clinical scientists do.
Multimodal AI for patient stratification and endpoint optimization: Integrating imaging, labs, digital biomarkers, and historical trial outcomes enables more precise cohort selection and improves the likelihood of detecting true therapeutic effect. These tools help convert today’s complex data streams into actionable insights.
Synthetic and hybrid control arms: While still emerging, these approaches reduce dependence on large traditional control cohorts by incorporating real-world evidence and model-generated comparators when appropriate. The result is faster recruitment and more efficient statistical design.
AI agents for operations: Operational agents can triage site queries, assist with eligibility adjudication, coordinate scheduling, and draft routine documentation. They are particularly helpful in reducing the administrative burden that slows trial execution.
The most underestimated category, and the one with the most long-term potential, is clinical-driven AI, where the model is trained to interpret clinical data the way a researcher with a PhD or a clinician would. This approach addresses the core issue of context, which is essential for decision-making in regulated environments.
From site-centric to data-centric trials
Trials are gradually evolving away from rigid site-based infrastructure and toward data-centric execution. AI accelerates this shift by enabling continuous monitoring, adaptive decision-making, and greater representation across diverse populations. The next phase of this transition requires progress in several areas:
- Reliable digital biomarkers collected via wearables and sensors that feed directly into the trial data ecosystem.
- Real-world evidence integration that allows trial designs to incorporate external data while maintaining regulatory rigor.
- Improved cohort diversity, supported by AI-driven recruitment models that identify and engage underrepresented populations.
- Always-on trial oversight, where adaptive protocols adjust based on real-time data rather than periodic interim reviews.
As these elements mature, trials will resemble dynamic learning systems rather than static sequences of predefined events.
Pharma cannot do this alone
The clinical-trial innovation ecosystem is now incredibly fragmented. A myriad of startups, many founded within the last five years, are attempting to solve different slices of the trial process. Some focus on recruitment; others on protocol simulation, operational automation, predictive enrollment, or digital biomarker analysis.
This fragmentation creates noise but also opportunity. The organizations that succeed will be those that adopt a hybrid strategy, in which internal data expertise is paired with carefully selected external partners. Evaluating early-stage companies requires disciplined technical assessment and an understanding of which partners can meet enterprise requirements in a regulated environment.
Pharma organizations also face a structural talent challenge. The best AI engineers often gravitate toward startups rather than large enterprises. This dynamic reinforces the need for partnership models that combine internal governance with external innovation rather than relying exclusively on one or the other.
What AI can (and cannot) fix
While AI can dramatically shorten timelines and improve decision-making, it is not a cure-all. It will not rescue a flawed trial design, replace human oversight, or eliminate the need for regulatory rigor. What it can do is accelerate the work around those elements, optimizing how protocols are developed, how patients are selected, how data is interpreted, and how milestones are achieved. The organizations that reap the greatest benefit will be those with disciplined data stewardship and a willingness to rethink long-held operational assumptions.
Erik Terjesen is the managing director at Silicon Foundry, a Kearney Company
The post Pharma’s Trial Problem: Outdated Systems, Broken Data, and the Coming AI Reset appeared first on GEN – Genetic Engineering and Biotechnology News.
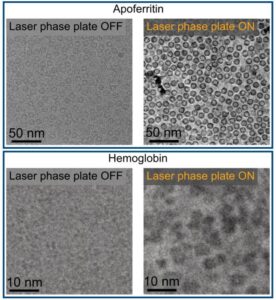
You know when you are at the eye doctor getting an updated prescription, and suddenly the world snaps into sharper focus? Physicists at the University of California (UC), Berkeley, have now done something similar for electron microscopy. By introducing phase contrast into a cryo‑electron microscope, they have delivered dramatically sharper images of some of biology’s smallest and most elusive proteins.
The advance comes from a new laser phase plate (LPP), described in the paper “Laser phase plate improves structure determination of small proteins by cryo‑EM,” which was published recently in Science. Led by physicist Holger Mueller, PhD, of UC Berkeley and Lawrence Berkeley National Laboratory, the team demonstrated that a laser‑driven phase plate can overcome one of cryo‑EM’s most persistent limitations: poor contrast for small proteins.
Cryo‑EM has transformed structural biology over the past decade, earning a Nobel Prize in 2017 for enabling high‑resolution structures without crystallization. But despite its impact, the technique still struggles with proteins below ~70 kilodaltons—a size range that includes about 90% of the human proteome. “Because of signal-to-noise limitations, the majority of human and animal proteins are too small to be analyzed by these methods [cryo-EM and cryoelectron tomography]. The increase in signal-to-noise ratio provided by this laser phase plate is expected to overcome these important limitations.”
The new LPP begins to address that problem. The LPP uses an intense, continuous‑wave laser to shift the phase of the electron beam itself. This produces true phase contrast without dimming or destabilizing the beam. Mueller described the laser focus as “75 kilowatts focused to a few microns… That’s more powerful than what you use for welding. It has more power than a military laser. It builds up the brightest continuous laser focus ever.”
Installed in a custom Thermo Fisher Titan Krios, the LPP immediately improved the clarity and resolvability of small proteins, including hemoglobin, which sits at the lower limit of what today’s cryo‑EM instruments can handle. As the authors wrote in the abstract: “Here, we show that the laser phase plate (LPP)… enhances the resolution in single-particle reconstruction of small proteins by improving specimen-motion correction, recovery of information from the early frames, as well as particle visualization, 3D classification, and alignment.”
These improvements were achieved using standard defocus ranges and reconstruction workflows. “For the most challenging cases—small particles, bad specimens—the laser produces a very considerable advantage,” Mueller said.
The impact extends beyond single‑particle analysis. Cryo‑electron tomography (cryo‑ET), which assembles multiple angular views of a molecule or protein into a three-dimensional image, stands to benefit even more. “With cryo-ET, we’re looking at small, very complicated cellular material that’s incredibly crowded inside the cell,” said Bridget Carragher, PhD, founding technical director of imaging at Biohub. “It’s like a forest of trees, and you’re trying to find one leaf on one tree in there. Cryo-ET needs a dramatic step forward in contrast, so we can start to see what’s going on inside the cell. That’s what the laser phase plate promises to give us.”
Biohub is developing a dual‑laser version of the system, designed to reduce component wear and minimize aberrations. Meanwhile, Mueller’s team is pushing toward imaging proteins as small as 17 kilodaltons, a threshold that would open access to vast regions of the human proteome previously invisible to cryo‑EM.
“This technology is a step function change for biology,” said Stephani Otte, PhD, Biohub’s vice president of imaging science. “What was once invisible will become visible—and that changes everything about how we understand disease.”
“The bottom line is, if you have a large protein and a really good sample—a fresh one or one frozen without bubbles, for example—you may not need the phase plate to get a single, high-quality image. But for a small protein and a bad sample, laser-on is best,” Mueller said. “This could fill an enormous gap in our knowledge of protein structures that can’t be crystallized or are too small for today’s cryo-EM. And it will be revolutionary for cryo-ET.”
The post Laser‑Driven Phase Contrast Enhances Cryo‑EM Resolution of Small Proteins appeared first on GEN – Genetic Engineering and Biotechnology News.
Uncategorized
STAT+: Updated: Tracking RFK Jr.’s promises to remake health in America
Updated June 11, 2026
WASHINGTON — A pledge to “Make America Healthy Again” earned Robert F. Kennedy Jr. his job atop U.S. health agencies a year and some change ago. He’s now had the opportunity to turn his words into action, with mixed results.
“All one needs” to prove the health secretary’s attentiveness is to “review my unprecedented list of accomplishments on a wide range of issues, all of which I drove,” Kennedy posted on X on Wednesday in response to a journalist.

Updated June 11, 2026
WASHINGTON — A pledge to “Make America Healthy Again” earned Robert F. Kennedy Jr. his job atop U.S. health agencies a year and some change ago. He’s now had the opportunity to turn his words into action, with mixed results.
“All one needs” to prove the health secretary’s attentiveness is to “review my unprecedented list of accomplishments on a wide range of issues, all of which I drove,” Kennedy posted on X on Wednesday in response to a journalist.
Can any of the new obesity medications in development stand out from the pack? Which company just broke records with its IPO? And will the Food and Drug Administration allow greater access to experimental peptides?
We discuss all that and more on this week’s episode of “The Readout LOUD,” STAT’s biotech podcast.


Illinois’ financial crisis could bring the state to a halt
The final 6 ‘Game of Thrones’ episodes might feel like a full season
New Season 8 Walking Dead trailer flashes forward in time
Mod turns ‘Counter-Strike’ into a ‘Tekken’ clone with fighting chickens
Meet Superman’s grandfather in new trailer for Krypton
Disney’s live-action Aladdin finally finds its stars

Laser‑Driven Phase Contrast Enhances Cryo‑EM Resolution of Small Proteins

STAT+: Updated: Tracking RFK Jr.’s promises to remake health in America

An obesity drug deep-dive, and peptides move mainstream

RFK Jr. claims his calendar is publicly available. We’ve been trying to get it for a year

Nonprofit buys experimental cancer drug to maintain patient access
Potential Cocaine Addiction Targets Identified Through Genetic Mapping in Rats
Illinois’ financial crisis could bring the state to a halt
The final 6 ‘Game of Thrones’ episodes might feel like a full season
New Season 8 Walking Dead trailer flashes forward in time
Mod turns ‘Counter-Strike’ into a ‘Tekken’ clone with fighting chickens
Meet Superman’s grandfather in new trailer for Krypton
Disney’s live-action Aladdin finally finds its stars
-
 Uncategorized9 years ago
Uncategorized9 years agoThese ’90s fashion trends are making a comeback in 2017
-
Uncategorized9 years ago
According to Dior Couture, this taboo fashion accessory is back
-
Endpoints News3 months ago
Novartis to pay $2B upfront to take next-gen PI3Kα inhibitor from Synnovation
-
Uncategorized9 years ago
Phillies’ Aaron Altherr makes mind-boggling barehanded play
-
Uncategorized9 years ago
Uber and Lyft are finally available in all of New York State
-
Contributors9 years ago
The final 6 ‘Game of Thrones’ episodes might feel like a full season
-
Uncategorized9 years ago
Steph Curry finally got the contract he deserves from the Warriors
-
Uncategorized9 years ago
The old and New Edition cast comes together to perform