GEN – Genetic Engineering & Biotechnology News
Leveraging the Full Potential of Regenerative Medicine Requires a Proactive Approach

Modern medicine has achieved extraordinary success in treating acute disease. Yet when it comes to chronic degenerative conditions, the diseases that dominate healthcare spending and disability in aging populations, our healthcare system remains fundamentally reactive.
Patients typically enter the medical system only after symptoms become severe enough to demand treatment. By that point, disease processes may have been progressing silently for years or even decades. Physicians are then left with a limited set of tools: manage symptoms, slow deterioration, or repair damage once it has already occurred.
This reactive model has shaped clinical practice, reimbursement systems, and regulatory frameworks for decades. But it is increasingly misaligned with what modern biology is teaching us about chronic disease. Many of the most prevalent conditions, including osteoarthritis, autoimmune disease, and metabolic disorders, develop through long periods of progressive biological dysfunction driven by inflammation, immune dysregulation, and gradual tissue degeneration.
By the time these diseases become clinically apparent, substantial damage may already be irreversible.
Regenerative medicine offers the potential to fundamentally change this trajectory. Advances in cell therapy, biologically active scaffolds, and tissue engineering are beginning to create therapeutic approaches that target the biological drivers of degeneration rather than simply treating downstream symptoms. But realizing this potential will require more than scientific innovation. It will require a shift in how healthcare systems think about disease intervention.

Regenerative therapies are unlikely to reach their full impact if they are introduced only after disease has advanced to late stages. Instead, these technologies are best suited to earlier intervention, i.e., when inflammatory signaling, immune dysregulation, and tissue degeneration can still be modulated before structural damage becomes permanent.
From the perspective of companies actively developing regenerative therapies, the challenge is not simply proving clinical efficacy; it is ensuring that healthcare systems are prepared to deploy these therapies at the stage of disease where they can deliver the greatest benefit.
In other words, regenerative medicine is not simply a new class of therapies. It represents an opportunity to move healthcare from a model centered on reactive treatment toward one focused on proactive disease modification.
The promise of regenerative medicine
Regenerative medicine encompasses a broad set of therapeutic approaches, including cell therapies, biologically active scaffolds, and gene-based technologies, designed to repair tissue or alter the biological processes that drive disease.
Among the most widely studied regenerative therapies are treatments derived from mesenchymal stromal/stem cells (MSCs). Rather than functioning primarily through direct tissue replacement, MSCs exert many of their therapeutic effects through paracrine signaling. These cells secrete cytokines, growth factors, extracellular vesicles, and other signaling molecules that influence immune activity and tissue repair mechanisms.1,2
These signaling pathways can affect several biological processes relevant to degenerative disease, including:
- Reduction of pro-inflammatory cytokine activity
- Modulation of immune cell signaling
- Alteration of catabolic and anabolic pathways in tissues
- Support of endogenous tissue repair mechanisms
Because these biological pathways operate early in many degenerative diseases, regenerative therapies may be most effective during the early to moderate stages of disease progression, when structural damage has not yet progressed beyond the body’s ability to maintain or restore tissue function.
This creates a therapeutic window in which regenerative interventions may slow degeneration, stabilize tissue function, or delay the need for invasive procedures—a therapeutic concept often described as disease modification.
Targeting inflammation-driven degenerative disease
Many chronic degenerative diseases share a common biological driver: persistent inflammation that gradually disrupts tissue homeostasis.
Osteoarthritis (OA) illustrates this process clearly. Once viewed primarily as a mechanical “wear-and-tear” condition, OA is now recognized as a complex disease involving inflammatory signaling pathways, synovial activation, and progressive cartilage degeneration.3
Regenerative therapies targeting the inflammatory microenvironment of the joint may help alter these pathways. Intra-articular MSC therapies, for example, are being studied for their ability to reduce inflammatory signaling and influence the balance between catabolic processes that degrade cartilage and anabolic processes that support tissue maintenance.
Several clinical studies have begun to demonstrate the therapeutic potential of MSC-based therapies in degenerative joint disease. In a multicenter randomized clinical trial comparing implantation of MSCs versus a hyaluronate gel with a microfracture procedure for large cartilage defects of the knee, patients receiving the MSC-based therapy showed significantly greater improvements in pain and functional outcomes over a five-year follow-up period.4
These findings illustrate how regenerative therapies may help stabilize degenerative processes before structural damage becomes advanced enough to require joint replacement.

A growing number of clinical programs are now exploring regenerative cell therapies for focal cartilage lesions and early OA—conditions that often precede the development of advanced joint degeneration. In these settings, biologic therapies designed to modulate inflammation and support cartilage repair may help stabilize the joint environment before extensive structural damage occurs.
If such approaches prove capable of delaying or preventing the need for joint replacement surgery, they could significantly alter the treatment paradigm for one of the most common causes of disability in aging populations.
At the same time, degenerative joint disease is multifactorial. In cases where OA results primarily from biomechanical abnormalities, such as chronic joint instability or abnormal loading patterns, those structural issues may need to be addressed before regenerative therapies can provide optimal benefit.
Immune modulation in autoimmune disease
The immunomodulatory properties of regenerative therapies also create potential applications in autoimmune disease.
Conditions such as multiple sclerosis, rheumatoid arthritis, and type 1 diabetes arise from dysregulated immune responses that target healthy tissue. Conventional therapies, including corticosteroids and biologic agents such as TNF inhibitors, typically act by suppressing specific components of the immune system.
Cell therapies such as MSCs may influence immune signaling through broader regulatory mechanisms. Preclinical and clinical research suggest that MSC therapies can modulate T-cell differentiation, promote regulatory T-cell activity, and influence macrophage polarization toward anti-inflammatory phenotypes.5
These mechanisms suggest regenerative medicine may offer the ability to recalibrate immune signaling networks rather than simply suppress them.
Despite rapid scientific progress, several structural barriers continue to limit the adoption of proactive regenerative medicine strategies in the United States. Healthcare delivery remains largely oriented around late-stage treatment rather than early biological intervention. Reimbursement systems, clinical guidelines, and regulatory reviews all influence when therapies are introduced in the treatment continuum.
Cultural and systemic attitudes toward healthcare also play a role. In many healthcare systems, treatment escalation occurs only after conservative therapies fail and symptoms worsen.

Japan provides an illustrative contrast in certain treatment pathways. For example, intra-articular hyaluronic acid injections are commonly used earlier in the treatment pathway for mild knee osteoarthritis in Japan. In the United States, clinical practice patterns vary widely and often reserve such interventions for later stages of disease progression.
More broadly, the economic case for prevention and early intervention continues to strengthen. Analyses from organizations such as Deloitte suggest that investments in prevention, early detection, and proactive health management could generate substantial long-term savings for healthcare systems. Realizing these benefits will require a structural shift toward earlier detection and earlier therapeutic intervention.
The future of regenerative medicine
The long-term promise of regenerative medicine lies not only in the development of new therapies but in the opportunity to rethink how healthcare approaches chronic disease.
For decades, medical innovation has focused largely on improving treatments for advanced disease. Yet many of the most prevalent conditions—degenerative joint disease, autoimmune disorders, and other chronic inflammatory conditions—are still typically treated only after significant biological damage has already occurred.
Regenerative medicine challenges this model. As our understanding of disease biology deepens, it is becoming increasingly clear that many chronic conditions progress through identifiable biological stages long before irreversible structural damage occurs. Advances in diagnostics, biomarkers, and imaging technologies may soon allow clinicians to detect these signals much earlier than has historically been possible.
When combined with therapies capable of modulating inflammation, immune signaling, and tissue repair, this creates the possibility of intervening earlier in disease progression—preserving function rather than attempting to restore it after it has already been lost.
However, achieving this vision will require more than scientific breakthroughs. Healthcare systems must adapt to support earlier intervention. Regulatory framework standards must continue to evolve to accommodate novel therapeutic modalities. Reimbursement frameworks must recognize the long-term value of disease modification rather than focusing exclusively on late-stage treatment.
Regenerative medicine should not be viewed as a miracle cure. But it represents one of the most promising opportunities to fundamentally change how medicine approaches degenerative disease. If responsibly developed and thoughtfully integrated into healthcare systems, regenerative therapies could help shift medicine toward a more proactive model, i.e., one focused on preserving health, maintaining function, and extending healthy lifespan.
For aging societies around the world, that shift may ultimately prove as important as any single medical breakthrough.
Ed Ahn, MD, is the CEO of Medipost.
References
1. Caplan AI, Correa D. The MSC: An injury drugstore. Cell Stem Cell. 2011;9(1):11–15. doi:10.1016/j.stem.2011.06.008
2. Pittenger MF, Discher DE, Péault BM, Phinney DG, Hare JM, Caplan AI. Mesenchymal stem cell perspective: cell biology to clinical progress. Science. 2019;363(6424):eaaw8730. doi:10.1126/science.aaw8730
3. Hunter DJ, Bierma-Zeinstra S. Osteoarthritis. The Lancet. 2019;393(10182):1745–1759. doi:10.1016/S0140-6736(19)30417-9
4. Lim HC, Park YB, Ha CW, Cole BJ, et al. Allogeneic Umbilical Cord Blood–Derived Mesenchymal Stem Cell Implantation Versus Microfracture for Large, Full-Thickness Cartilage Defects in Older Patients: A Multicenter Randomized Clinical Trial and Extended 5-Year Clinical Follow-up. Orthopaedic Journal of Sports Medicine. 2021;9(1):2325967120973052.
5. Uccelli A, Moretta L, Pistoia V. Mesenchymal stem cells in health and disease. Nature Reviews Immunology. 2008;8(9):726–736. doi:10.1038/nri2395
The post Leveraging the Full Potential of Regenerative Medicine Requires a Proactive Approach appeared first on GEN – Genetic Engineering and Biotechnology News.
GEN – Genetic Engineering & Biotechnology News
Bioengineered Implants Deliver Multi-Drug Therapy in Animal Models
In a new paper, scientists from Northwestern University and their collaborators at Rice University and Carnegie Mellon University report on their progress towards developing so-called implantable “living pharmacies.” These are tiny devices containing engineered cells that continuously produce medicines inside the body. Details of the study, which was done in rats, are published in Device in a paper titled “Design of a wireless, fully implantable platform for in-situ oxygenation of encapsulated cell therapies.”
The device, which is called the hybrid oxygenation bioelectronics system for implanted therapy or HOBIT, is roughly the size of a folded stick of gum. It integrates engineered cells with oxygen-producing bioelectronics and is designed in such a way that the cells are shielded from the body’s immune system while also receiving oxygen and nutrients needed to keep them alive and producing drugs for several weeks. In the future, these devices could be deployed to treat chronic conditions without requiring patients to carry, inject, or remember to take medications.
“This work highlights the broad potential of a fully integrated biohybrid platform for treating disease,” said Jonathan Rivnay, PhD, a professor of biomedical engineering and materials science and engineering at Northwestern and a co-principal investigator of the project. “Traditional biologic drugs often have very different half-lives, so maintaining stable levels of multiple therapies can be challenging. Because our implanted ‘cell factories’ continuously produce these biologics, keeping the cells alive with our oxygenation technology allows us to sustain steady levels [of] multiple different therapeutics at once.”
Solving the oxygenation challenge was critical to the success of HOBIT. When engineered cells are packed together in an implant, they compete for oxygen to live. Without a steady supply, many cells die, which limits how much medicine the implants can produce. In an earlier study, Rivnay and his collaborators demonstrated how a tiny electrochemical device could generate oxygen by splitting nearby water molecules, and showed that supplying oxygen locally dramatically improved the survival of implanted therapeutic cells. The latest iteration of their device integrates that oxygen-generation technology in a fully implantable, wireless system.
Digging into the details of the device, HOBIT contains three primary components: a cell chamber that holds the genetically engineered cells, a miniature oxygen generator, and electronics and a battery to regulate oxygen production and wirelessly communicate with external devices. Because the device produces oxygen directly inside the implant, the cells receive a steady supply even in hypoxic environments. “We are producing oxygen directly where the cells need it,” Rivnay said. “That allows us to support much higher cell densities in a much smaller space.” In fact, “cell densities in HOBIT were roughly six times higher than conventional unoxygenated encapsulation approaches.”
According to the paper, the team engineered the cells to produce three different biologics—an anti-HIV antibody, a GLP-1-like peptide used to treat type 2 diabetes, and leptin, a hormone that regulates appetite and metabolism. They implanted the devices under the skin of rats and monitored drug levels in their bloodstreams for 30 days. Blood measurements of animals with the implanted devices showed sustained levels of all three biologics throughout the study period. In contrast, in animals that were implanted with devices without oxygenation, the biologics that had shorter half-lives were undetectable by the seventh day. Drugs with longer half-lives in these animals also declined steadily over time. At the end of the testing period, roughly 65% of the cells in the oxygenated devices remained viable compared with roughly 20% in control devices.
For their next steps, the scientists intend to test their devices in larger animal models and explore disease-specific applications, including therapies based on transplanted pancreatic cells. “As these technologies continue to develop, devices like this could eventually act as programmable drug factories inside the body—delivering complex therapies in ways that simply aren’t possible today,” Rivnay said.
The post Bioengineered Implants Deliver Multi-Drug Therapy in Animal Models appeared first on GEN – Genetic Engineering and Biotechnology News.
GEN – Genetic Engineering & Biotechnology News
Gut-Immune Link Identified in Multiple Sclerosis-Related Neuroinflammation
Multiple sclerosis (MS) is a debilitating neurological disorder caused by malfunctioning immune responses that target the brain and spinal cord of the central nervous system (CNS). New research led by Shohei Suzuki, MD, PhD, assistant professor, division of gastroenterology and hepatology, and Tomohisa Sujino, PhD, associate professor, School of Medicine, at Keio University, Japan, has now indicated how the gut can initiate neuroinflammation in multiple sclerosis.
Their study found that intestinal epithelial cells (IECs) promote the development of pathogenic T cells that migrated to the spinal cord and induced disease symptoms in mouse models of the disorder.
The researchers examined intestinal tissues from patients with MS and mice with experimental autoimmune encephalomyelitis (EAE), a close analog of MS. In both cases, they observed an increase in TH17 cells and an upregulation of major histocompatibility complex class II (MHC II) expression in IECs. Deleting MHC II in IECs reduced the accumulation of TH17 cells in the gut and lowered the severity of EAE. They suggest the results could inform future strategies for developing targeted therapeutics against autoimmunity.
“While current therapies for MS often target B cells, our study highlights the gut as an important therapeutic site,” Suzuki commented. “Modulating intestinal microbiota or antigen-presenting activity of IECs represents new approaches to treating autoimmune neurological diseases.”
Suzuki, Sujino, and colleagues reported on their findings in Science Immunology, in a paper titled “Intestinal Epithelial MHC Class II Induces Encephalitogenic CD4⁺ T Cells and Initiates Central Nerves System Autoimmunity,” in which they concluded, “Our findings reveal an interaction between gut IECs and neuroinflammatory diseases through MHC II expression in human MS and mouse EAE, providing a mechanistic link between gut immune education and CNS autoimmunity and opening new avenues for targeting intestinal immunity in neuroinflammatory diseases.
Failure of the immune system to distinguish ‘self’ from ‘non-self’ entities leads to excessive autoimmune responses against self-proteins like myelin, which forms a protective covering on the neurons. Multiple factors influence the onset and progression of MS, including genetic susceptibility, environmental triggers, and, more recently, the gut microenvironment. Patients with MS exhibit alterations in their gut microbiota, while the gut microbiota and microbial metabolites play a pivotal role in shaping the chronic autoreactive immune responses. “… in an experimental autoimmune encephalomyelitis (EAE) model, commensal or specific microbes were found to be essential for disease initiation and progression,” the authors wrote.
However, in trying to define this gut–CNS axis, the cellular mechanisms that relay the gut-derived signals to the immune system to influence autoimmune inflammation in the CNS remain poorly understood. “Increasing evidence shows that the gut microbiota influences neurological diseases such as Parkinson’s, Alzheimer’s, and MS,” Sujino stated. “However, the mechanisms linking gut microbes, intestinal immunity, and brain inflammation remain unclear. We were keen to identify how gut immune responses contribute to neuroinflammatory diseases.”
Prior research has shown that gut-derived signals can promote the differentiation of T cells into pathogenic T helper 17 (TH17) in mouse models of MS. Recent studies have suggested that IECs can function as antigen presenting cells that help induce these pathogenic cells, but the underlying mechanisms have been unclear.
Building on their previous observation that mild intestinal (ileal) inflammation exists in experimental autoimmune encephalomyelitis (EAE), which is a mouse model of MS, the authors set out to test whether similar inflammation is present in patients with MS. By performing single-cell RNA sequencing on intestinal biopsies, the team identified that inflammatory Th17 cells accumulate in the mouse EAE model as well as in the intestine of patients with MS, suggesting a conserved gut–CNS axis that may be active in human diseases.
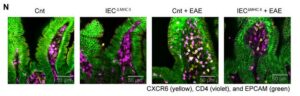
In both EAE mice and patients with MS, intestinal epithelial cells upregulated antigen presentation pathways. Particularly, epithelial cells in the ileum had higher expression of major histocompatibility complex class II (MHC II) that presents antigens to CD4+ T cells. “Clinically, patients with MS exhibited an increased expression of epithelial MHC II–associated genes and an accumulation of CD4 T cells in the small intestine, suggesting the conservation of this gut-CNS axis in human diseases,” the scientists stated. Experiments showed that selective deletion of MHC II in IECs reduced pathogenic Th17 cell generation and disease severity. “Conditional deletion of MHC II in IECs showed that epithelial antigen presentation was indispensable for the local expansion of pathogenic Th17 cells in the gut and their subsequent migration to the CNS,” the team stated.
![Immunofluorescence analysis was performed on terminal ileum samples from Cnt, IECΔMHCII, Cnt + EAE, and IECΔMHCII + EAE mice. A total of 3–5 tissue sections were analyzed per mouse, with 3 mice included in each group. [Shohei Suzuki]](https://www.genengnews.com/wp-content/uploads/2026/03/low-res-2-1-300x96.jpeg)
mouse, with three mice included in each group. [Shohei Suzuki]
IECs do not typically present antigens to immune cells. So, the team conducted co-culture assays to test the antigen presentation function of IECs. Their findings demonstrate that IECs can directly present antigens in an MHC II-dependent manner to prime CD4+ T cells in the gut. Notably, in these assays, IECs induced Th17 polarization of activated CD4+ T cells. It became clear that the gut was a critical site for immune activation of pathogenic CD4+ T cells that polarized into pro-inflammatory Th17 cells. “These findings provide direct functional evidence that IEC-expressed MHC II is sufficient to drive Th17 polarization from primed CD4 T cells in an antigen-dependent manner, supporting a direct role for IECs as non-professional antigen-presenting cells,” the scientists reported.
To investigate whether the Th17 cells directly contribute to the pool of autoreactive cells in the CNS, they used transgenic mice that express the Kaede protein, which undergoes photoconversion from green to red fluorescence upon exposure to violet light. This model allowed for precise tracking of pathogenic Th17 cells induced in the intestinal lamina propria that then migrate to the spinal cord and drive neuroinflammation.
Taken together, the study findings reveal a critical role for MHC II expressed by IECs in the expansion of pathogenic Th17 cells that subsequently migrate to the CNS during EAE, providing a mechanistic link between gut immune responses and autoimmune neuroinflammatory diseases. The results demonstrate that while systemic circulation allows T cell exchange across immune tissues, the epithelial–immune interactions within the gut mucosal compartment can essentially shape effector T cell responses in the brain.
“This study reveals a previously unknown role of IECs in antigen presentation and Th17 programming, thereby defining a gut-CNS immunological axis with important implications for understanding and treating autoimmune neuroinflammation,” the authors concluded. “Our findings suggest that the modulation of epithelial antigen presentation could serve as a novel therapeutic approach for MS and related diseases. Given the accessibility of the gut epithelium to dietary, microbial, and pharmacological interventions, targeting IEC–T cell interactions may offer a tractable strategy for immunomodulation.”
The post Gut-Immune Link Identified in Multiple Sclerosis-Related Neuroinflammation appeared first on GEN – Genetic Engineering and Biotechnology News.
GEN – Genetic Engineering & Biotechnology News
Agentic AI, Virtual Cell, LNP Vaccine Boosters, Engineered Organs, and Mergers
This week, agentic AI steps into the limelight buoyed by the momentum from generative AI. And there’s a new virtual cell model in town courtesy of AI-drug developer Xaira Therapeutics. From the frontiers of AI, our discussion turned to feats of engineering in regenerative medicine and lipid nanoparticles. In one study, scientists redesigned LNPs to avoid the liver and accumulate in the lymph nodes. In the other, efforts to develop and implant a lab grown esophagus from donor pigs bear fruit. Finally, Novartis plans to spend up to $3 billion to expand its cancer pipeline with the acquisition of Pikavation Therapeutics. And Merck is acquiring Terns Pharmaceuticals for approximately $6.7 billion also with an eye towards boosting its cancer portfolio.
Listed below are links to the GEN stories referenced in this episode of Touching Base:
NVIDIA GTC 2026: Agentic AI Inflection Hits Healthcare and Life Sciences
By Fay Lin, PhD, GEN Edge, March 18, 2026
Xaira’s First Virtual Cell Model Is Largest To-Date, Toward Complex Biology
By Fay Lin, PhD, GEN Edge, March 25, 2026
Modified Lipid Nanoparticles Boost mRNA Vaccine Delivery to Lymph Nodes
GEN, March 24, 2026
Engineered Esophagus Rebuilds Missing Organ Segment in Pig Models
GEN, March 20, 2026
Novartis Acquires Pikavation for Up to $3B, Expanding Cancer Pipeline
GEN, March 22, 2026
Merck Bolsters Cancer Pipeline with $6.7B Terns Buyout
By Alex Philippidis, GEN Edge, March 25, 2026
Touching Base Podcast
Hosted by Corinna Singleman, PhD
Behind the Breakthroughs
Hosted by Jonathan D. Grinstein, PhD
The post Agentic AI, Virtual Cell, LNP Vaccine Boosters, Engineered Organs, and Mergers appeared first on GEN – Genetic Engineering and Biotechnology News.


Illinois’ financial crisis could bring the state to a halt
The final 6 ‘Game of Thrones’ episodes might feel like a full season
New Season 8 Walking Dead trailer flashes forward in time
Mod turns ‘Counter-Strike’ into a ‘Tekken’ clone with fighting chickens
Meet Superman’s grandfather in new trailer for Krypton
Disney’s live-action Aladdin finally finds its stars
Gilead Swallows Another Partner, Paying up to $5B for ADC Specialist Tubulis

STAT+: Pharmalittle: We’re reading about FDA backing domestic production, another Gilead deal, and more
FDA Seeks Expanded Authority To Regulate Postapproval Manufacturing Changes
Sanofi Bispecific Scores in Asthma, Rhinosinusitis, but Eczema Bet Doesn’t Pay Off

STAT+: Gilead to buy cancer biotech Tubulis for more than $3 billion
Gilead continues dealmaking streak with $3.15B Tubulis buy for ADCs
Illinois’ financial crisis could bring the state to a halt
The final 6 ‘Game of Thrones’ episodes might feel like a full season
New Season 8 Walking Dead trailer flashes forward in time
Mod turns ‘Counter-Strike’ into a ‘Tekken’ clone with fighting chickens
Meet Superman’s grandfather in new trailer for Krypton
Disney’s live-action Aladdin finally finds its stars
-
 Uncategorized9 years ago
Uncategorized9 years agoThese ’90s fashion trends are making a comeback in 2017
-
Contributors9 years ago
The final 6 ‘Game of Thrones’ episodes might feel like a full season
-
Uncategorized9 years ago
According to Dior Couture, this taboo fashion accessory is back
-
Uncategorized9 years ago
The old and New Edition cast comes together to perform
-
Uncategorized9 years ago
Phillies’ Aaron Altherr makes mind-boggling barehanded play
-
Uncategorized9 years ago
Uber and Lyft are finally available in all of New York State
-
Uncategorized9 years ago
Disney’s live-action Aladdin finally finds its stars
-
Uncategorized9 years ago
Steph Curry finally got the contract he deserves from the Warriors