GEN – Genetic Engineering & Biotechnology News
Judge’s Halt on RFK Jr.’s Vaccine Changes Remains in Effect, At Least for Now
Brian Murphy, a U.S. District Judge in Massachusetts, recently temporarily blocked key parts of RFK Jr.’s plan to change the U.S. childhood vaccine schedule. Judge Murphy sided with medical groups who maintained that changes could reduce vaccination rates and threaten public health.
The vaccine issue represents the latest attempt by the Trump team that will further negatively impact U.S. healthcare and research. The administration has already slashed funding for scientific institutions, restricted research grants, and weakened public health infrastructure.
To get expert insight on the national importance of the judge’s decision, GEN spoke to Tyler B. Evans, MD, co-founder, CEO, and principal investigator at the Wellness Equity Alliance, a national group of public health leaders. He is also the author of Pandemics, Poverty, and Politics: Decoding the Social and Political Drivers of Pandemics from Plague to COVID-19.
GEN: What does this ruling mean for public health and vaccine confidence?
Evans: This ruling reinforces the foundational principle that vaccine policy in the U.S. must be developed through a structured, evidence-based process involving qualified independent experts, as defined by the Federal Advisory Committee Act. The court found that 13 of Secretary Kennedy’s 15 ACIP appointees likely lacked the scientific and medical qualifications required by federal standards, that the government offered no substantive scientific rationale for departing from decades of established immunization process, relying instead on a presidential directive, and that the CDC exceeded its authority by reducing recommended childhood vaccinations from 17 diseases to 11 without consulting the advisory committee.
The childhood vaccine schedule is the product of decades of rigorous, peer-reviewed science. It is not discretionary guidance. When the process used to develop it is bypassed, the integrity of the recommendations themselves is compromised. This ruling restores the requirement that the process be followed. Whether it holds through appeal will determine how much institutional credibility can be recovered.
For the vaccine development community specifically, this ruling has implications beyond the immediate policy question. The mRNA platform that produced the COVID-19 vaccines is the foundation for a generation of pipeline candidates targeting RSV, influenza, cancer, and rare diseases. When the federal advisory process that evaluates and recommends these products is destabilized, it introduces regulatory uncertainty that affects investment decisions, clinical development timelines, and the willingness of researchers and companies to commit resources to vaccine innovation.
GEN: Why are childhood vaccine schedules designed as population-level prevention systems, not individual consumer choices?
Evans: Vaccines work at two levels simultaneously. They protect the individual child who receives them, and they protect the community around that child by reducing the overall circulation of the pathogen. That second function, population-level immunity, is what prevents outbreaks. It is what keeps a child undergoing chemotherapy for leukemia, whose immune system is too compromised to receive a vaccine, from sitting next to a classmate carrying measles. It is what protects a two-week-old infant who is too young for their first dose but entirely dependent on everyone around them being vaccinated.
When we treat the vaccine schedule as a menu of personal preferences, we are not just accepting risk for one child. We are degrading the collective protection that keeps preventable diseases from regaining a foothold. The schedule is sequenced and timed the way it is because the data tells us when children are most vulnerable to specific diseases and when their immune systems will mount the most effective response. It is an engineered system, not a buffet. Reducing it from 17 recommended diseases to 11 without scientific justification does not give parents more choice. It gives pathogens more opportunity.
GEN: How can policy uncertainty around vaccine recommendations undermine public trust and lower vaccination rates?
Evans: The evidence on this point is already accumulating. Twenty-six states have rejected CDC vaccine guidance over the past year. Kindergarten DTaP [diphtheria, tetanus, and acellular pertussis] vaccination coverage has declined from 95% in the 2019-20 school year to 92.1% in 2024-25, falling below the threshold needed to sustain herd immunity for several vaccine-preventable diseases. A JAMA Network Open study examining 149,000 children in Ohio during the 2025 measles outbreak found MMR [measles, mumps, and rubella] vaccination rates below the 93% threshold needed to prevent sustained transmission. These are not projections. They are measurements of what is already happening.

I have spent four decades working in communities where trust in public health infrastructure was already fragile. What I can tell you from that experience is that uncertainty is more damaging than almost any specific policy decision. When parents see the federal government change the vaccine schedule, then a court blocks those changes, then the administration signals it will fight back, what registers is not the details of any single ruling. What registers is instability.
And in the absence of clarity, people default to inaction. They delay. They skip appointments. They wait to see what happens next. And as a result, we see vaccination rates decline. They decline, not through dramatic refusal but through quiet hesitation. The damage from this kind of policy whiplash is cumulative and difficult to reverse because once a parent decides to wait, re-engaging them requires a level of trust that the system has already spent.
GEN: What are the potential public health consequences, including the return of preventable diseases, if routine immunization coverage declines?
Evans: The consequences are not hypothetical. We are already seeing them. The measles outbreak that began last year now threatens elimination status in the Americas. The Pan American Health Organization (PAHO) has scheduled a formal review of the U.S. and Mexico’s elimination status for later this year after the region as a whole lost its measles-free designation in November 2025. As of March 2026, the CDC has confirmed over 1,300 measles cases in the U.S. this year alone, on top of more than 2,200 in 2025, the highest annual total in over three decades. Ninety-three percent of confirmed cases have been in unvaccinated individuals or those with unknown vaccination status.
Pertussis cases in the U.S. have surged from roughly 7,000 in 2023 to over 35,000 in 2024, with at least 13 deaths in 2025. The majority of pertussis deaths historically occur in unvaccinated or incompletely vaccinated infants, and the deaths reported in 2025 followed that pattern. These are not deaths caused by a novel pathogen we do not understand. They are deaths from a disease we effectively controlled for decades through the very immunization infrastructure that is now being undermined.
The math of herd immunity is precise. Measles requires roughly 95% vaccination coverage to prevent sustained transmission. When coverage drops even a few percentage points below that threshold, outbreaks become inevitable, and they concentrate in the communities with the lowest vaccination rates, which are often the same communities facing the greatest barriers to healthcare access.
I run street medicine and primary care programs for people living in shelters, encampments, and transitional housing. I have seen what happens when infectious disease enters a community with no buffer of population immunity, no reliable access to testing, and no clear pathway to treatment. It moves fast, and it moves through the people with the fewest options first.
If routine childhood immunization rates continue to decline, the consequences will not be distributed evenly. They will land first and hardest in the communities that were already underserved before the first dose was skipped. And when those communities need a public health response, they will be at the back of the line, because they always are.
The post Judge’s Halt on RFK Jr.’s Vaccine Changes Remains in Effect, At Least for Now appeared first on GEN – Genetic Engineering and Biotechnology News.
GEN – Genetic Engineering & Biotechnology News
Bioengineered Implants Deliver Multi-Drug Therapy in Animal Models
In a new paper, scientists from Northwestern University and their collaborators at Rice University and Carnegie Mellon University report on their progress towards developing so-called implantable “living pharmacies.” These are tiny devices containing engineered cells that continuously produce medicines inside the body. Details of the study, which was done in rats, are published in Device in a paper titled “Design of a wireless, fully implantable platform for in-situ oxygenation of encapsulated cell therapies.”
The device, which is called the hybrid oxygenation bioelectronics system for implanted therapy or HOBIT, is roughly the size of a folded stick of gum. It integrates engineered cells with oxygen-producing bioelectronics and is designed in such a way that the cells are shielded from the body’s immune system while also receiving oxygen and nutrients needed to keep them alive and producing drugs for several weeks. In the future, these devices could be deployed to treat chronic conditions without requiring patients to carry, inject, or remember to take medications.
“This work highlights the broad potential of a fully integrated biohybrid platform for treating disease,” said Jonathan Rivnay, PhD, a professor of biomedical engineering and materials science and engineering at Northwestern and a co-principal investigator of the project. “Traditional biologic drugs often have very different half-lives, so maintaining stable levels of multiple therapies can be challenging. Because our implanted ‘cell factories’ continuously produce these biologics, keeping the cells alive with our oxygenation technology allows us to sustain steady levels [of] multiple different therapeutics at once.”
Solving the oxygenation challenge was critical to the success of HOBIT. When engineered cells are packed together in an implant, they compete for oxygen to live. Without a steady supply, many cells die, which limits how much medicine the implants can produce. In an earlier study, Rivnay and his collaborators demonstrated how a tiny electrochemical device could generate oxygen by splitting nearby water molecules, and showed that supplying oxygen locally dramatically improved the survival of implanted therapeutic cells. The latest iteration of their device integrates that oxygen-generation technology in a fully implantable, wireless system.
Digging into the details of the device, HOBIT contains three primary components: a cell chamber that holds the genetically engineered cells, a miniature oxygen generator, and electronics and a battery to regulate oxygen production and wirelessly communicate with external devices. Because the device produces oxygen directly inside the implant, the cells receive a steady supply even in hypoxic environments. “We are producing oxygen directly where the cells need it,” Rivnay said. “That allows us to support much higher cell densities in a much smaller space.” In fact, “cell densities in HOBIT were roughly six times higher than conventional unoxygenated encapsulation approaches.”
According to the paper, the team engineered the cells to produce three different biologics—an anti-HIV antibody, a GLP-1-like peptide used to treat type 2 diabetes, and leptin, a hormone that regulates appetite and metabolism. They implanted the devices under the skin of rats and monitored drug levels in their bloodstreams for 30 days. Blood measurements of animals with the implanted devices showed sustained levels of all three biologics throughout the study period. In contrast, in animals that were implanted with devices without oxygenation, the biologics that had shorter half-lives were undetectable by the seventh day. Drugs with longer half-lives in these animals also declined steadily over time. At the end of the testing period, roughly 65% of the cells in the oxygenated devices remained viable compared with roughly 20% in control devices.
For their next steps, the scientists intend to test their devices in larger animal models and explore disease-specific applications, including therapies based on transplanted pancreatic cells. “As these technologies continue to develop, devices like this could eventually act as programmable drug factories inside the body—delivering complex therapies in ways that simply aren’t possible today,” Rivnay said.
The post Bioengineered Implants Deliver Multi-Drug Therapy in Animal Models appeared first on GEN – Genetic Engineering and Biotechnology News.
GEN – Genetic Engineering & Biotechnology News
Gut-Immune Link Identified in Multiple Sclerosis-Related Neuroinflammation
Multiple sclerosis (MS) is a debilitating neurological disorder caused by malfunctioning immune responses that target the brain and spinal cord of the central nervous system (CNS). New research led by Shohei Suzuki, MD, PhD, assistant professor, division of gastroenterology and hepatology, and Tomohisa Sujino, PhD, associate professor, School of Medicine, at Keio University, Japan, has now indicated how the gut can initiate neuroinflammation in multiple sclerosis.
Their study found that intestinal epithelial cells (IECs) promote the development of pathogenic T cells that migrated to the spinal cord and induced disease symptoms in mouse models of the disorder.
The researchers examined intestinal tissues from patients with MS and mice with experimental autoimmune encephalomyelitis (EAE), a close analog of MS. In both cases, they observed an increase in TH17 cells and an upregulation of major histocompatibility complex class II (MHC II) expression in IECs. Deleting MHC II in IECs reduced the accumulation of TH17 cells in the gut and lowered the severity of EAE. They suggest the results could inform future strategies for developing targeted therapeutics against autoimmunity.
“While current therapies for MS often target B cells, our study highlights the gut as an important therapeutic site,” Suzuki commented. “Modulating intestinal microbiota or antigen-presenting activity of IECs represents new approaches to treating autoimmune neurological diseases.”
Suzuki, Sujino, and colleagues reported on their findings in Science Immunology, in a paper titled “Intestinal Epithelial MHC Class II Induces Encephalitogenic CD4⁺ T Cells and Initiates Central Nerves System Autoimmunity,” in which they concluded, “Our findings reveal an interaction between gut IECs and neuroinflammatory diseases through MHC II expression in human MS and mouse EAE, providing a mechanistic link between gut immune education and CNS autoimmunity and opening new avenues for targeting intestinal immunity in neuroinflammatory diseases.
Failure of the immune system to distinguish ‘self’ from ‘non-self’ entities leads to excessive autoimmune responses against self-proteins like myelin, which forms a protective covering on the neurons. Multiple factors influence the onset and progression of MS, including genetic susceptibility, environmental triggers, and, more recently, the gut microenvironment. Patients with MS exhibit alterations in their gut microbiota, while the gut microbiota and microbial metabolites play a pivotal role in shaping the chronic autoreactive immune responses. “… in an experimental autoimmune encephalomyelitis (EAE) model, commensal or specific microbes were found to be essential for disease initiation and progression,” the authors wrote.
However, in trying to define this gut–CNS axis, the cellular mechanisms that relay the gut-derived signals to the immune system to influence autoimmune inflammation in the CNS remain poorly understood. “Increasing evidence shows that the gut microbiota influences neurological diseases such as Parkinson’s, Alzheimer’s, and MS,” Sujino stated. “However, the mechanisms linking gut microbes, intestinal immunity, and brain inflammation remain unclear. We were keen to identify how gut immune responses contribute to neuroinflammatory diseases.”
Prior research has shown that gut-derived signals can promote the differentiation of T cells into pathogenic T helper 17 (TH17) in mouse models of MS. Recent studies have suggested that IECs can function as antigen presenting cells that help induce these pathogenic cells, but the underlying mechanisms have been unclear.
Building on their previous observation that mild intestinal (ileal) inflammation exists in experimental autoimmune encephalomyelitis (EAE), which is a mouse model of MS, the authors set out to test whether similar inflammation is present in patients with MS. By performing single-cell RNA sequencing on intestinal biopsies, the team identified that inflammatory Th17 cells accumulate in the mouse EAE model as well as in the intestine of patients with MS, suggesting a conserved gut–CNS axis that may be active in human diseases.
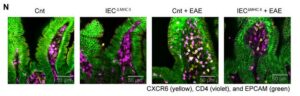
In both EAE mice and patients with MS, intestinal epithelial cells upregulated antigen presentation pathways. Particularly, epithelial cells in the ileum had higher expression of major histocompatibility complex class II (MHC II) that presents antigens to CD4+ T cells. “Clinically, patients with MS exhibited an increased expression of epithelial MHC II–associated genes and an accumulation of CD4 T cells in the small intestine, suggesting the conservation of this gut-CNS axis in human diseases,” the scientists stated. Experiments showed that selective deletion of MHC II in IECs reduced pathogenic Th17 cell generation and disease severity. “Conditional deletion of MHC II in IECs showed that epithelial antigen presentation was indispensable for the local expansion of pathogenic Th17 cells in the gut and their subsequent migration to the CNS,” the team stated.
![Immunofluorescence analysis was performed on terminal ileum samples from Cnt, IECΔMHCII, Cnt + EAE, and IECΔMHCII + EAE mice. A total of 3–5 tissue sections were analyzed per mouse, with 3 mice included in each group. [Shohei Suzuki]](https://www.genengnews.com/wp-content/uploads/2026/03/low-res-2-1-300x96.jpeg)
mouse, with three mice included in each group. [Shohei Suzuki]
IECs do not typically present antigens to immune cells. So, the team conducted co-culture assays to test the antigen presentation function of IECs. Their findings demonstrate that IECs can directly present antigens in an MHC II-dependent manner to prime CD4+ T cells in the gut. Notably, in these assays, IECs induced Th17 polarization of activated CD4+ T cells. It became clear that the gut was a critical site for immune activation of pathogenic CD4+ T cells that polarized into pro-inflammatory Th17 cells. “These findings provide direct functional evidence that IEC-expressed MHC II is sufficient to drive Th17 polarization from primed CD4 T cells in an antigen-dependent manner, supporting a direct role for IECs as non-professional antigen-presenting cells,” the scientists reported.
To investigate whether the Th17 cells directly contribute to the pool of autoreactive cells in the CNS, they used transgenic mice that express the Kaede protein, which undergoes photoconversion from green to red fluorescence upon exposure to violet light. This model allowed for precise tracking of pathogenic Th17 cells induced in the intestinal lamina propria that then migrate to the spinal cord and drive neuroinflammation.
Taken together, the study findings reveal a critical role for MHC II expressed by IECs in the expansion of pathogenic Th17 cells that subsequently migrate to the CNS during EAE, providing a mechanistic link between gut immune responses and autoimmune neuroinflammatory diseases. The results demonstrate that while systemic circulation allows T cell exchange across immune tissues, the epithelial–immune interactions within the gut mucosal compartment can essentially shape effector T cell responses in the brain.
“This study reveals a previously unknown role of IECs in antigen presentation and Th17 programming, thereby defining a gut-CNS immunological axis with important implications for understanding and treating autoimmune neuroinflammation,” the authors concluded. “Our findings suggest that the modulation of epithelial antigen presentation could serve as a novel therapeutic approach for MS and related diseases. Given the accessibility of the gut epithelium to dietary, microbial, and pharmacological interventions, targeting IEC–T cell interactions may offer a tractable strategy for immunomodulation.”
The post Gut-Immune Link Identified in Multiple Sclerosis-Related Neuroinflammation appeared first on GEN – Genetic Engineering and Biotechnology News.
GEN – Genetic Engineering & Biotechnology News
Agentic AI, Virtual Cell, LNP Vaccine Boosters, Engineered Organs, and Mergers
This week, agentic AI steps into the limelight buoyed by the momentum from generative AI. And there’s a new virtual cell model in town courtesy of AI-drug developer Xaira Therapeutics. From the frontiers of AI, our discussion turned to feats of engineering in regenerative medicine and lipid nanoparticles. In one study, scientists redesigned LNPs to avoid the liver and accumulate in the lymph nodes. In the other, efforts to develop and implant a lab grown esophagus from donor pigs bear fruit. Finally, Novartis plans to spend up to $3 billion to expand its cancer pipeline with the acquisition of Pikavation Therapeutics. And Merck is acquiring Terns Pharmaceuticals for approximately $6.7 billion also with an eye towards boosting its cancer portfolio.
Listed below are links to the GEN stories referenced in this episode of Touching Base:
NVIDIA GTC 2026: Agentic AI Inflection Hits Healthcare and Life Sciences
By Fay Lin, PhD, GEN Edge, March 18, 2026
Xaira’s First Virtual Cell Model Is Largest To-Date, Toward Complex Biology
By Fay Lin, PhD, GEN Edge, March 25, 2026
Modified Lipid Nanoparticles Boost mRNA Vaccine Delivery to Lymph Nodes
GEN, March 24, 2026
Engineered Esophagus Rebuilds Missing Organ Segment in Pig Models
GEN, March 20, 2026
Novartis Acquires Pikavation for Up to $3B, Expanding Cancer Pipeline
GEN, March 22, 2026
Merck Bolsters Cancer Pipeline with $6.7B Terns Buyout
By Alex Philippidis, GEN Edge, March 25, 2026
Touching Base Podcast
Hosted by Corinna Singleman, PhD
Behind the Breakthroughs
Hosted by Jonathan D. Grinstein, PhD
The post Agentic AI, Virtual Cell, LNP Vaccine Boosters, Engineered Organs, and Mergers appeared first on GEN – Genetic Engineering and Biotechnology News.


Illinois’ financial crisis could bring the state to a halt
The final 6 ‘Game of Thrones’ episodes might feel like a full season
New Season 8 Walking Dead trailer flashes forward in time
Mod turns ‘Counter-Strike’ into a ‘Tekken’ clone with fighting chickens
Meet Superman’s grandfather in new trailer for Krypton
Disney’s live-action Aladdin finally finds its stars
Gilead Swallows Another Partner, Paying up to $5B for ADC Specialist Tubulis

STAT+: Pharmalittle: We’re reading about FDA backing domestic production, another Gilead deal, and more
FDA Seeks Expanded Authority To Regulate Postapproval Manufacturing Changes
Sanofi Bispecific Scores in Asthma, Rhinosinusitis, but Eczema Bet Doesn’t Pay Off

STAT+: Gilead to buy cancer biotech Tubulis for more than $3 billion
Gilead continues dealmaking streak with $3.15B Tubulis buy for ADCs
Illinois’ financial crisis could bring the state to a halt
The final 6 ‘Game of Thrones’ episodes might feel like a full season
New Season 8 Walking Dead trailer flashes forward in time
Mod turns ‘Counter-Strike’ into a ‘Tekken’ clone with fighting chickens
Meet Superman’s grandfather in new trailer for Krypton
Disney’s live-action Aladdin finally finds its stars
-
 Uncategorized9 years ago
Uncategorized9 years agoThese ’90s fashion trends are making a comeback in 2017
-
Contributors9 years ago
The final 6 ‘Game of Thrones’ episodes might feel like a full season
-
Uncategorized9 years ago
According to Dior Couture, this taboo fashion accessory is back
-
Uncategorized9 years ago
The old and New Edition cast comes together to perform
-
Uncategorized9 years ago
Phillies’ Aaron Altherr makes mind-boggling barehanded play
-
Uncategorized9 years ago
Uber and Lyft are finally available in all of New York State
-
Uncategorized9 years ago
Disney’s live-action Aladdin finally finds its stars
-
Uncategorized9 years ago
Steph Curry finally got the contract he deserves from the Warriors